
Chiropractic Treatment During Pregnancy
It’s time to get into why a lot of expecting ladies find me and my practice in Bedford, NH. If they aren’t already getting checked and adjusted during pregnancy pro-actively to optimize their delivery outcomes and/or the seemingly inevitable back pain, sciatic pain, and hip pain of pregnancy – then they are in my office because they have a breech baby.
About 3-4% of full-term pregnancies will get a breech diagnosis at the time of 34 weeks of gestation and onward. Most head up fetuses can flip spontaneous to head down before 34 weeks. This abnormal fetal positioning is confirmed on ultrasound and can be concerning as it is likely to result in dystocia (difficult birth, typically caused by a large or awkwardly positioned fetus). Breech presentation past the 34th week of pregnancy is one of the most common reasons for scheduled c-section deliveries. I’m no OBGYN or labor and delivery nurse, but here are some of the various breech presentations for a visual. (I’m not going to get into all the various fetal presentations, just the ones that can relate to Webster Technique).

The importance of preventing these subsequent cesarean section deliveries is important considering current statistics in this country. In the US in 1965 when c-section rates were first recorded, we were delivering 4.5% of our babies through this surgical intervention. The rate has increased annually. The rates for 2020 per the CDC are now topping 38.1%! [1]
Nearly 15% of these c-sections are being performed because of the breech presentation. In 1985 the World Health Organization (WHO) proposed 15% as the highest acceptable limit for cesarean section rates.[2] This figure was based on the cesarean section rates of countries with the lowest perinatal mortality rates. The US is falling well short of these limits.
With all that being said, let’s get into what the Webster Technique is and how it works. The Webster technique was developed by the late Dr. Larry Webster, D.C. Dr. Webster was the founder of what is today known as the International Chiropractic Pediatric Association (ICPA). Dr. Webster developed the technique that now bears his name to address what he called “intrauterine constraint”. By reducing some of the neuroanatomical stresses being applied to the mother’s uterus, the baby would be given more of an opportunity to move into the proper head down position on their own. This approach has proven to be much less traumatic than the obstetric approach, known as external cephalic version, and much more effective as well.[3]
Intrauterine constraint as it relates to this technique, is the result of abnormal forces and stresses being applied to the uterus. For this to make sense let’s review some basic anatomy of the female pelvis. The pelvic basin consists of the left and right inominate bones (the large hip bones) and the sacrum (“tailbone”). The uterus is held in place within the pelvic basin by various sets of ligaments, we are going to focus on the uterosacral ligament and the round ligaments.
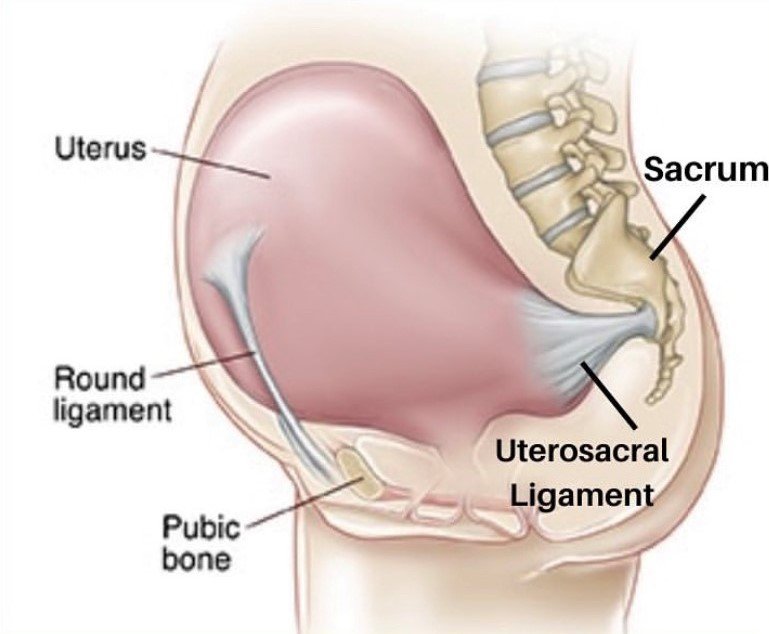
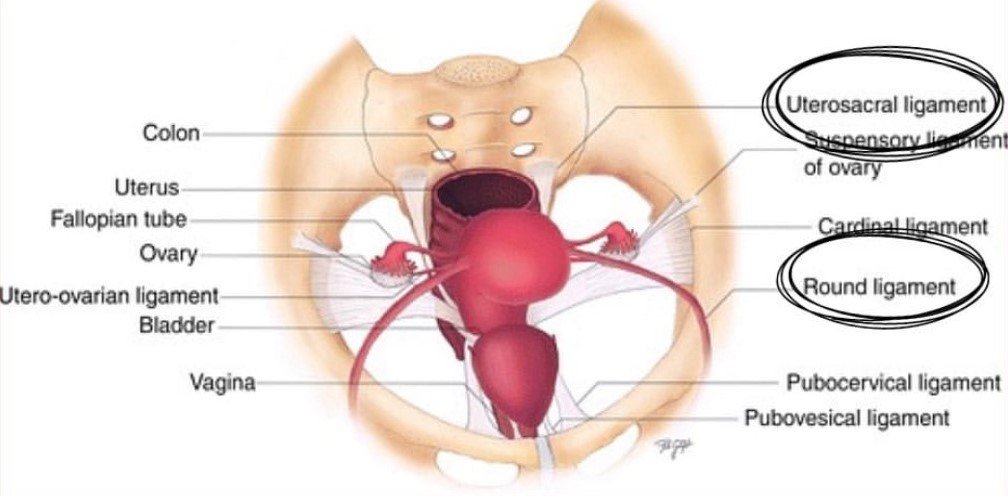
The uterosacral ligament attaches the back of the uterus to the sacrum aka “tailbone” while the round ligaments anchor the front lateral corners of the uterus. The round ligaments are rope-like bands of connective tissue that support the uterus (womb). The scientific term for this round ligament is the gubernaculum, funny word right? Just to not confuse anyone there is a round ligament of the liver but clearly, we are focusing our discussion on anatomy lower in the body.
Ok, back to it. When the sacrum is misaligned within the pelvic basin it can pull on these ligaments in an unequal fashion which can contribute to distortion in the position of the uterus within the pelvis. This distortion is what causes Dr. Webster referred to as “intrauterine constraint”. Essentially the uterus can be “torqued” for last of a better word, which can reduce the uterine space available for the developing fetus to move around in. If the fetus can’t move freely during the mother’s 34th week of pregnancy, they may not be able to get into the head down position on their own resulting in the breech presentation.
The most important thing I need to stress here is that THE WEBSTER TECHNIQUE IS NOT A BABY TURNING TECHNIQUE! I repeat, it is not a baby turning technique.
The Webster Technique is a specific chiropractic sacral analysis and diversified adjustment. The goal of the adjustment is to reduce the effects of the sacral subluxation / SI joint dysfunction. In doing so, neurobiomechanical function in the pelvis is facilitated.
The analysis and adjustment for all expecting mother’s is safe, non-invasive, comfortable and easy. Most of my mom’s are SUPER excited that they get the opportunity to lay on their belly again while pregnant. This is done in my office with pregnancy pillows placed on the adjusting table. After the sacrum is adjusted, then we always finish by doing some work on the appropriate round ligament to help reduce and mitigate any tension through it as a result of the sacral misalignment.


Sacral subluxation/misalignment may contribute to difficult labor for the mother (ex dystocia), caused by inadequate uterine function, pelvic contraction and baby mal-presentation. Correction of sacral subluxation may have a positive effect on all of these causes of dystocia.
Last thing, the Webster Technique can only be administered by a licensed chiropractor who has also had additional education and training through the ICPA (International Chiropractic Pediatric Association). If you’re not local but would love to find a Doc who specializes in this like I do, you can search for one here:
https://icpa4kids.com/find-a-pediatric-chiropractor/
Learn more about treatment during pregnancy & postpartum at Precision Chiro
References:
[1] https://www.cdc.gov/nchs/data/nvsr/nvsr70/nvsr70-17.pdf
[2] https://apps.who.int/iris/bitstream/handle/10665/161442/WHO_RHR_15.02_eng.pdf
[3] https://icpa-research.s3.amazonaws.com/webster_technique_definition.pdf